
In this post John Davis returns to discussing the cataclysmic health issues he encountered in the USA and critiques some of the care he received. It is difficult to criticise health professionals during the Corona Crisis. Hence, the example’s provided below should be understood within the context of the earlier articles in these series that have highlighted the huge appreciation, love and respect that John holds for the professionals who saved his life. However, any system will have flaws and this week’s article sets out to highlight the need for health professionals to not lose sight of their kinder selves when they feel under pressure during this epidemic.
A deficit approach to health issues locates our health outcomes in relation to flaws with in our behaviours, personalities and identities, rather than understanding the societal causes of ill health. In previous articles in this blog we have have employed the ‘Glasgow Effect Report’ to demonstrate how the structure and organisation of society causes and perpetuates ill health. The Glasgow effect report connected ill health to 60 years of Westminster and local political mismanagement of housing policy that broke up support networks, isolated people and dis-empowered them. Lesley Riddoch’s book Blossom shows us that communities that took over their tenements and collectively organised, experienced improved health outcomes.
The lesson for the current crisis is that localism heals and enables people to confront sources of ill health, but, what kills us is: national politics that reinforce inequality, miserly bureaucrats that fail to prepare properly for a crisis and politicians that delay decisions because they are too concerned with political dogma, the media and the great ‘English’ pint (as one newspaper called it when questioning the need for the shutdown of pubs).
The social model teaches us not to blame ill-health on the individual. Never in our lifetime has such a distinction been so important. The Corona Virus is spread by individuals but many of the deaths it causes are preventable. Poverty, lack of access to health care, delayed social responses and political inertia (particularly during February and early March) means the UK curve is now the worst in Europe and has resulted in (at least) 32,065.deaths (indeed the Financial Times claimed today that the UK death rate is 50,000 above average figures for the same period over the last 5 years) . At the start of the outbreak mapping suggested that it could be possible, with the correct government approach, to keep the UK deaths below 20,000. The UK Government will have to answer for why the death rate has been so high.

As you can see from the chart, the UK death toll is now above that of Spain and Italy. In the early days of the outbreak, when I listened to a Westminster Government News Conference, I was concerned about the reflexive ability of the ‘experts’ that were on the TV, day after day, pontificating about their slide rules, mapping, curves, data and predictions. Of most concern were discussions about the pros and cons of heard immunity – it should not have required ‘experts’ to tell the UK government that a heard-mentality was dangerous. Common sense tells us that a sheep like mentality often misses important details and there is no doubt that comments like ‘take it on the chin’ were stupid, cavalier and reprehensible. The initial leadership at UK level was confused and contradictory and after a period of clarity, the statement this Sunday about going back to work, has again led to confusion and sent out a mixed message.
We should have had a clear message about the need to isolate much earlier in this process and had much stronger testing, tracking and isolation. The lack of capacity for testing was not an accident, it was the result of UK Government decisions to ignore their own mock emergency work which highlighted their lack of preparedness for a pandemic.
The situation we find ourselves in, is that we have been unable to use local public health services and officers to get on top of this epidemic because the Tories (initially with the help of the Liberals) have spent ten years cutting local services and breaking up the local structures that connect health and social care services. In particular, the privatisation of elderly care has been a disaster in term of preventing a national response and questions need to be posed about the extent to which Tory cuts in local authorities and repressive cultures of management in local authorities have left us unable to respond quickly to the pandemic (these questions need to be posed in Scotland as well – in terms of whether devolution resulted in a different approaches or whether the same cultures of local cuts and mismanagement also resulted in increased deaths)
There was something too inhuman and academic about the early discussions involving the UK Government. Most of my friends went into isolation before the lockdown. We had worked out for ourselves, whilst the UK Prime Minister was dithering, that the only way to stop this thing was to isolate. We had received social media correspondence from friends in Italy and the Basque region which, basically, advised us to ignore the politician’s lack of response and to take our own steps to self-isolate.
Scotland’s curve is much better than England, but slightly worse than Wales and the North of Ireland.

I worry for England. Each statistic is a person (and their loved ones) who went through an unimaginable loss, a loss where you were not able to see your loved ones at the end. It gives me no comfort to state that, at present, Scotland maps below England. We should not jump to any conclusions. Indeed, the stats could just be related to density of population, vagaries in recording of cause of death and inadequate record collection. My only proviso would be that with higher levels of poverty and inequality in Scotland, you would expect Scotland to map above England – so maybe something different happened here?
The issue of the Corona Virus is beyond party politics. In time, enquiries will tell us whether politicians, whatever their party, made decisions that saved lives. At the moment you can draw your own conclusions about which politicians are doing their job right.
I have the utmost respect for Nicola Sturgeon but our current politics are always judged with the benefit of hind sight. Nicola has been much easier to follow on TV than the UK politicians and has been clear and candid about the fact that she has probably made mistakes and that we have an issue with how the virus has spread in care homes. However, even I realise that whilst we can try to practice a non-judgemental approach and understand the pressures politicians, health systems and care homes are under, in the end, the politician’s will be judged on their record. Because, that’s how politics works.
I think the difference in Nicola’s approach is summed up by how, even in the darkest moments, she does not come across as pompous and manages to balance a sober attitude with a human touch e.g. Nicola made me laugh (at the start of this process before the death toll became evident) when she re-posted Janey Godley’s voice over of her press conference.
Humour helps in a crisis but, in article 6 of this series I questioned whether our gallows humour had prevented myself and my wife being more honest about our feelings and created longer term communication problems. I love my wife very much and nothing could ever change that – she is and will always will be the mother of my three fantastic children. She gave me hope when I was at my lowest in the hospital, even when we did not see eye to eye on everyday things.
This series of articles have connected the humorous way that we approached our experience in Phoenix with our sense of Scottishness. Indeed, whilst trying to grasp the extent of my surgery and subsequent impairments, our Scots terminology caused the medics some problems. After the first operation I asked the doctors, ‘is ma tackle in tact – like, still there?’ Tackle not being a term for your manhood in Arizona, this question caused much confusion and subsequent laughter.
I could not feel nor see what and where the surgeons had cut things off – all I could feel was an overwhelming pain. I had two drains sticking out of each hip, which contributed to me being unable to move. I had to lie on large square pads made out of a sort of nappy/diaper material and as I explained in a previous post, my dressings had to be changed every two hours.
At first, I couldn’t move at all, but after a while I could move my arms to lift things close to me (like the buzzer on the intercom system which was mainly used to ask the nurses to turn me, change the pads or administer more drugs when their effect was wearing off). Over time, I would work out really inventive ways to lasso things I had dropped on the flour or staff had slightly moved out of reach. Every moment where I developed a slightly greater range of movement enabled a quiet sense of euphoria.
As I progressed the word shoogle got a lot of mileage, as in, ‘Can I just shoogle over rather than have you guys move me and put the pain up tae high doe’. The staff laughed a lot at that one and even more when I told them you could also use the term shoogle to chastise tight people at the bar when it comes for their turn ‘on the bell’ (to pay) and you have to watch them overly labour the task of finding their wallet in their pockets, as in, ‘Whilst you shoogle, I’ll pay’.
One day a staff member came in and said, ‘I am here to change your chucks’. This put my wife and myself into hysterics. My wife had to explain that, in Scotland, chucks were another term for the parts of your tackle that dangle down and that since these parts had survived the operation, a change of the pads would be fine but I would quite like to keep my chucks, thank you very much.’
Initially, my and my wife’s sense of humour had lots of benefits as it cheered me up, demonstrated our ability to laugh in the face of adversity and illustrated our willingness to resist what life threw at us. But, as the days ground on, it became more difficult to sustain a humorous approach. And, it is important that, as the Corona Crisis journeys on, we balance our sense of humour with a sober approach that pays respect to those who have been taken by the virus.
Lessons in Scots apart, the dressing/pad changes were excruciating. The gods only know what it would have been like if the infection had progressed from back to front and my tackle had not survived. But, equally, had I been in the same situation as the patient that my wife had encountered, who had lost his tackle, I would have just had to grin and bear it and get on with adjusting to the impact of that impairment in whatever way was possible.
That is the thing about life. A friend of mine says, ‘Life is a fucking ‘bitch’’ and you have to get on with it. Setting aside the gendered nature of the word ‘bitch’, he is right, I had no other choice than to endure and try as best as I could to survive my ordeal. That is what ‘No hierarchy of impairment means’, we find a way to live whatever is happening to us, for as long as we can.
I was unlucky to have picked up such a rare infection. Yet, I was lucky because I was taken to the best hospital in Phoenix and then had a great intensive care team and was subsequently placed on one of the best wards in the hospital. At night times and weekends the staff ratios could be problematic and you could be left in a lot of pain. But, the staff always explained what was going on (it is professional to own up to your limitations) and having worked in a lot of education, health, and social service settings, I was able to approach their difficulties with an empathetic mind.
The most prevalent issue facing staff concerned the inability of managers to do their job. Management mistakes with rotas are the bane of health care workers lives. They create staff shortages where experienced staff member are left with a handful of less experienced staff. A couple of times, I became aware that staff members had changed or taken on extra shifts to ensure I was cared for properly and that my chances of reinfection were kept to a minimum. And, this is the type of selflessness that we are seeing day in day out during the Corna Virus. We see the best in people coming out and we need to ensure that we build a new politics from that – that supports everyone, however they are hustling, on the basis that, as this song by Forest Sun says, we are not failures or saviours, we are all, just, stubborn breathing hearts – like you:
Just me and the moon
In this whole big night
Trying to get in tune
Trying to get right…
I am not the one you turn to anymore
I don’t know what you are going through
I am not a failure, I’m not a savior
I am a stubborn breathing heart like you
Everybody’s hustling
Trying to make it through
We all feel that gnawing hunger
For something new
I tried to connect with all the stubborn breathing hearts I encountered in the USA. Some of the kindest nurses included younger junior and trainee nurses who were extremely good at their job and did extra shifts to improve their practice. Some of the issues we experience concerning health care practice are not always about a person’s years’ service but about how a person builds their experience, how quickly they can adapt their practice and how willing they are to change things to ensure patients receive the care that they require.
Junior staff can quickly become good at their jobs if they have a supportive environment and we, in a generous way, share our experiences with them. At the moment the Corona Virus crisis has resulted in newly trained medics being rushed into post – they will require support to be at their best and also the correct equipment to reduce the stress they feel.
When I work with professionals I am keen to impress upon them that they can always improve their practice, no one is a finished item and that you are never to old or young to learn new things. I always apply that same philosophy to my own self.
It is presently difficult to be critical of health care staff but it is important that we voice our criticisms if, we want the health system to improve. One of my worst moments, after the operations, occurred when the mobile x-ray folk came. One of them, in order to get his boards under me, lifted me like a sack of tatties and plonked me back down. Then, after the x-ray, he removed the boards in a manner that could only cause maximum pain – it was like he had got his quota to do and had no time for niceties.
I had had x-rays and scans done when I came into the hospital and the staff had been so considerate. Hence, the mobile guy’s behaviour was a shock and a lesson for me that not all staff worked to the same standards. What struck me was that, from the start, he avoided eye contact, never introduced himself by name and did not smile when he approached me.
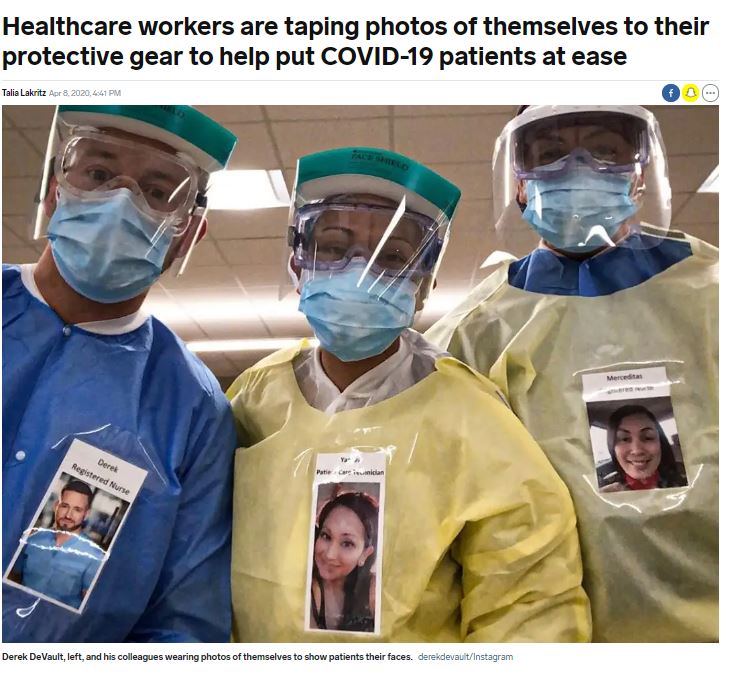
When I worked in a children’s hospital, the children explained to me that the first thing a medic had to do was treat them like a human being, tell them their name and demonstrate a friendly or funny side. It struck me that this advice is also useful for those working with adults. We have to avoid losing are humanity during moments of crisis and I was cheered when I recently saw that ICU staff were now pinning pictures of themselves to their protective clothing – so that patients could identify with them on a more personal level:
I have also been aware, through my work on anti-discrimination, that when we create social distance, when we treat another person as an inanimate object (such as a sack of tatties), when we cage people in ‘camps’ and/or ostracise them from our communities; then it is easier to do harmful things to them. The x-ray guy couldn’t look me in the eye because he knew what he was about to do to me and did not want to be held to account. He did not introduce himself because it would have made a connection. He did not smile because he did not want to build a relationship.
Article 6 hinted at the fact that, despite my attempts to put my best foot forward, I was not always able to be at my best. It was hard to for me to be myself when the pain was so overwhelming. My son spoke to me on the phone and told me to always say to the staff, who used a 1 to 10 pain scoring number scale, that the pain was a ten, as otherwise, ‘they muck around with your pain killers’. I laughed at his advice, the pain was always ten and above, so this was easy to do. The scoring only has meaning when you can say a number lower than ten. Sadly, I lived in the land of ten and above for far too long. A friend had texted me that one day the pain would get better and that I should work with the staff to try different medication options – that advice kept me going and did help.
The hardest things post-op were learning to walk again, having dressings changed, toileting, having IV drips, having cannulas changed, and having restrictions over showering – which I could not do without supervision because I was a fall risk. The tubes for drips and taking bloods were moved regularly until I hardly had a vein in my lower arms that hadn’t been used. The staff were happy when I remember where some good veins where between my elbow and wrist that used to stick out after I had done weight training.
It was funny how the smallest things really cheered me up in the hospital. I was so chuffed when the nurse flicked away at the area of my arm that I had suggested and the vein emerged. The lesson I draw from this is that, when we are at our weakest and most vulnerable, we do not remove the standards that ensure that health and social care staff are still enabled to do the small things for us that matter. When we are in a crisis we have to keep our humanity, it is all that patients have left when they are stripped down to nothingness.
The drips and machines regularly woke me during the night. Every time an IV bag emptied an alarm went off. It reminded me of, 4 years before, when I had cared for my son, when he had had life threatening surgery – the machines on the ward drove the young people to distraction. Can it really be beyond our technological ability to design a less fucking noisy process of health care? Neither myself nor my son were physically able to switch off these machines (though it was possible for a patient to do so if they had the manoeuvrability).
This is a reasonable adjustment that should be made for disabled people in hospital. It can’t be right that some patients are able to shut the machines up and others are not – for me, the machine noises are a way of demonstrating the totalising power of the hospital, it’s a benign dictatorship and all that bleeping is there to send the message – the medics are in charge. For some people, particularly visitors, the ‘medics are in charge’ stuff might be a comforting thought. For the patients the noises just create anxiety, restlessness and headaches.
Going to the toilet was a ridiculously difficult process, especially during the day when staff were continuously coming in and out of the room. In a very dumb-ass male way, my personal side assumed there could be such a thing as privacy in a hospital. My work side knew this not to be true. At night the chance of reinfection was worrisome when staff were unavailable to change the dressings.
You could hear the staff dashing along the corridor to an emergency just when your needs for a dressing change, medication or a bed pan reached its peak. In the most pain ridden of nights, all you could do was find a place of escape in yourself, a favourite memory, song or moment and wait it out till help was at hand. The song Playing Old Records by Erin Viancourt, with the line ‘I think sad songs make me better, so I aint gonny put them away’, kinda captures the nature of this process – where I would just put my headphones on, and try and escape, until help was at hand:
Being assessed as a fall risk, meant I had to wear a coloured band on my arm and my bed was alarmed so that if, during my delirious moments, I moved towards the rails (getting beyond the rails was physically impossible in the early days) – the staff would know and check on me. I was given socks to wear for when I got up to do my daily exercises, indeed, you can see the socks in this photo:

The board at the bottom of the bed was very important. It had goals set on it (mine for that day were rest/sleep and pain control), on the right side there were timings concerning the two painkillers that I was prescribed Narco and Gabapentin. I was able to buzz the staff if, for any reason, they missed the next timing and the board helped in some way put you at the centre of your pain control.
Loads of staff had computer trolleys (I did not see such things in UK hospitals), there was a pull out monitor on the wall which the consultants and senior nurses pulled out to show me my test scores which really helped to place you at the centre of your healthcare. There was a TV, which I did not use much. You could plug your headphones into the buzzer handset and listen to the TV which meant that the room and ward was sometimes much quieter than others I had experienced.
I got into a routine of bloods, pain killers, breakfast, physio/OT, water, dressings, injections, bed-wash (sometimes shower), lunch, O2/blood pressure testing, sleeping, evening meal, physio/OT etc. It is notable that I had two bouts of working with Physios or OTs most days – in the UK I may not have received such generous physio/OT support.
Managing the gaps between pain killers became a zen like experience where I tricked my mind with all sorts of stuff, but, sometimes I had nothing left and a long time to go before the next relief – short breathing, meditation, signing and rocking/moaning to the rhythm of the pain had to fill those gaps.
Most staff, when they came on shift, put their pager number up on the board on the wall. I never used the phone to call them. I pressed the buzzer and if they didn’t come I figured someone with more needs than me was being attended to, or, they were on a well-deserved break. I trusted that when they could be there for me, they would be.
I wasn’t allowed to bend, so sitting on the toilet was out and I also had problems because for a couple of months I couldn’t feel anything other than overwhelming pain below my waist – so being touched to be cleaned by a nurse or have dressings changed was sheer hell. Eventually, I became an expert at what worked and was very vocal to new staff about the process in a kind of, ‘please work with me, there is an easy and a hellish way to do this’ way.
In the main, the staff worked extremely well with me but on one occasion, to my shame, I did lose it whilst I was having my dressings changed. I slightly raised my voice to a nurse assistant who gripped me overly harshly. I moaned through my painful scream: ‘I can nae suffer you to touch me like that, that’s no way to treat another human being, get off me’. Considering, I could hardly move myself, and I was on my side naked from the waist down with only a towel to cover my manhood, It wasn’t the cleverest moment to finally make a complaint. She could have done anything she liked to me. But, it is testimony to her dignity that she immediately left the room and asked another nurse, who knew the process well, to sort my dressings.
The next day this less than gentle nurse assistant was also assigned to me and I looked up sheepishly with faintly apologetic eyes when she came in – she just nodded hello and went about her business of checking my fluids. She seemed very calm and professional, I heard later that she had said to another nurse that my complaint wasn’t a problem and indeed it was to be expected because I’d been through so much. Such generosity. She had not judged me by my worst moment on my worst day, but empathetically understood what I had been through.
I was right to try and stop the pain but I should have done it in a less male way – if I had said, ‘I realise you haven’t done this before, it is very tricky, could you ask your colleague to show you’, I probably would have got to the same end point, in a much nicer way. But the problem for me was that the pain was like nothing you could imagine. It is hard to be cerebral when your whole nervous system is suddenly shot excruciatingly into action.
I regretted my grumpy behaviour towards the nursing assistant and tried to learn a lesson to be more patient. I rarely, if ever, felt angry with staff. What little energy I had, went into trying to work out how to avoid as many moments of agony as was possible. Over time, I tried to use my experience of campaigning in the 2014 independence referendum to help me to bring forward a calmer self. During that campaign we were often attacked verbally and sometimes physical (e.g. by middle aged men who would spit at us on their way back from their jobs in the banking industry). We learned to stay calm whilst under fire.
We used the metaphor of a butterfly to bolster our peaceful approach. Our campaign was not built on a rigid hierarchy it involved lots of different people, lots of peaceful butterflies working their beautiful wings to making the winds of change move. To this day, my friends and I still send each other messages with blue butterflies in them as symbols of hope.
My great friend Marian Corker, who was deaf, a feminist and a lesbian, once gave me the signing name, ‘The Butterfly Collector’ because I kept introducing her to beautiful and intelligent women that I was lucky enough to be friends with. It was a nice sign name to have, but, unlike a Butter Fly Collector, I have no need to capture such beauty and intelligence in a jar, nor to pin such elegance on a page. I prefer to see butterflies as gentle and beautiful symbols of resistance, that help us to out manoeuvre the darker things in life. So, in time, I tapped into my better self, tapped into my inner butterfly , tried to be as nice as possible and, I think, most of the staff greatly appreciated the way I worked with them.
This post has sought to explain the trickiness of the daily routine of the hospital, has highlighted the need for health professional to never loose their human touch and has called on you to understand that we are all just stubborn breathing hearts who are trying to endure what life throws at us. In so doing, it has encouraged you to avoiding judging your-self or other people by our worst moments of our worst days. The Corona Virus is bringing a lot of bad news – we need to look for the best in each other if we are to endure and come out the other side.
Thanks for reading this post, tune in next time for Article 8 and a discussion of an incident that occurred with a less than reflexive plastic surgeon that highlights the need to avoid letting other people define who you are and the need, quite literally, to turn the other cheek.
You have been reading an article from the Don’t Let Me Die In Phoenix Series. Follow the links below to access the other articles in this series.
Don’t Let Me Die In Phoenix Article 1 An 8-1 Dog In A Two Horse Race
Don’t Let Me Die In Phoenix Article 2: ‘He Was Aye Working!’
Don’t Let Me Die In Phoenix Article 3: His Legs Were Weak And His Back Was Bent
Don’t Let Me Die In Phoenix Article 4: Walk Not Alone Among The Flames
Don’t Let Me Die In Phoenix Article 5 The Partial From The Whole:
Don’t Let Me Die In Phoenix Article 6 Everybody Hurts:
Don’t Let Me Die In Phoenix Article 7: Don’t Judge Us By Our Worst Moment Of Our Worst Day
Don’t Let Me Die In Phoenix Article 8: If He Wiz Chocolate He’d Eat Himsel’
Don’t Let Me Die In Phoenix Article 9: ‘It Doesn’t’ Have To Be ‘Right’ To be Called Love’
Don’t Let Me Die In Phoenix Article 10: It’s Hard Tae Catch A breath When Yir Daein’ Mair Fir Less
Don’t Let Me Die In Phoenix Article 11: The Cherry Blossoms of Home
Don’t Let Me Die In Phoenix Article 12: Come Home
Don’t Let Me Die In Phoenix Article 13 Epilogue – ‘Yir a Lang Time Hauf Deed!’
What We Can Learn From The ‘Don’t Let Me Die In Phoenix’ Series About Post-Traumatic Stress:
Categories: Uncategorized
